Get the weekly SPARTANAT newsletter.
Your bonus: the free E-Book from SPARTANAT.

With Hard Bandages (4): The Three Tactical Phases
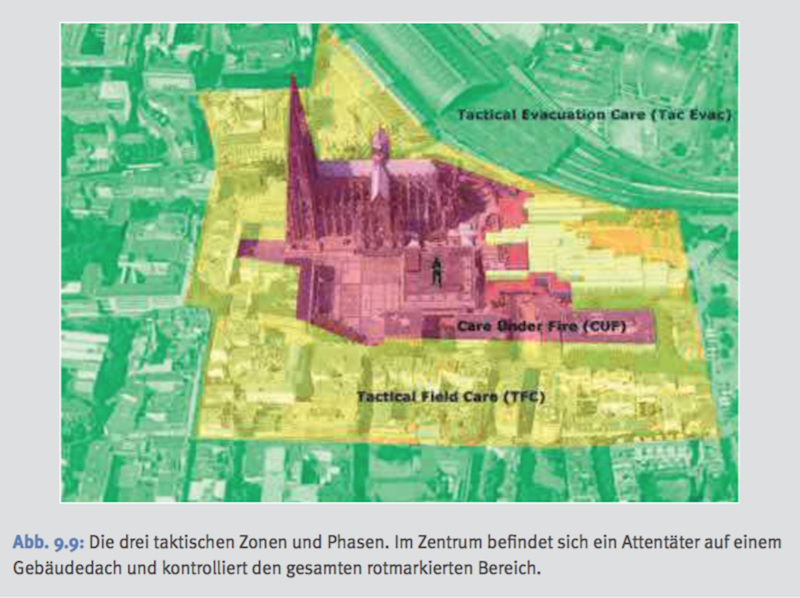
TCCC/TEMS structure consists of three tactical phases - red zone (CUF), yellow zone (TFC), and green zone (TEC), each with specific actions and priorities. In the red zone, first responders focus on neutralizing armed opponents and providing essential emergency medical care. In the yellow zone, treatment is carried out in cover away from gunfire, with considerations for ballistic protection. Green zone focuses on evacuation care once the immediate danger is eliminated. Coordination and communication are vital throughout all phases to ensure efficient response and care.

 Red/Hot Zone - Care Under Fire (CUF)
Immediate measures at the scene of the attack under fire
From the armed opponent, there is an immediate danger to the life or limb of all those present on-site. This includes already wounded individuals, potential rescuers, as well as uninvolved individuals. In the red zone, unarmed emergency services personnel should not be present in principle. An exception would of course be accidental presence during an attack or a deliberate attack on emergency medical infrastructure, such as hospitals or ambulance teams.
The top priority for first responders in the red zone is the quickest possible avoidance of the present danger. This goal can be achieved by incapacitating the armed opponent. In other words, they are killed or seriously wounded so that they can no longer continue their actions. Another possibility would be for the offender to leave the scene due to the resistance. Depending on the scenario, it is also conceivable that the police forces may initially be unable to eliminate or displace the enemies. But they could support the evacuation of the wounded from the immediate danger area by providing covering fire. This is intended to keep the enemy down and allow evacuation teams to approach the wounded and transport them to suitable cover for further treatment.
This all requires coordinated action from the first responders. So they must return fire and communicate at the same time.
With the control center or similar:
Call for help. Where am I? How does the situation look like? Request reinforcements and rescue forces.
With your tactical unit:
A wounded colleague is at the front left at the corner of the house. Perpetrator with a long gun, entrenched behind a wall at 2 o'clock (in other words, from your location seen from the front right). Provide cover, I'll get the wounded.
With the wounded:
Crawl behind the corner of the house! How are you injured? Use your tourniquet! It's in your left leg pocket! We'll get you out as soon as we can!
In the red zone, the Care Under Fire phase, neutralizing the perpetrators is top priority as long as they can continue to hinder personnel at the attack site. As many personnel as possible must engage in the gunfight, with as few as necessary approaching the wounded. Medical measures are limited to the absolute essentials. Ideally, the wounded themselves seek cover and treat their injuries in the initial attack. Following the principle: If everyone helps themselves, everyone is helped. Stopping life-threatening, massive extremity bleeding by applying a tourniquet is, if anything, the only feasible emergency medical action in the red zone. And as noted above, ideally by the wounded themselves. If the victims of the attack are not trained gun carriers but unaware citizens, self-treatment is likely to be ruled out in most cases.
Essentially, it is crucial for the first responders to minimize the time spent at the immediate attack site. The top principle here is: "Do not burden your team by becoming a victim yourself!" This means that an approach to the wounded may need to be postponed if it poses a significant risk to the rescuer. Prioritization of casualties should be done before or during the approach, especially in scenarios with multiple casualties. Critically wounded individuals who are not in life-threatening conditions may need to be disregarded to treat those with a higher chance of survival, given the ongoing firefight. Triage is consciously avoided at this point since patient selection can only be very rough at this time and mainly occurs at a distance (remote assessment). It is conceivable that the nearest wounded individual to the rescuers is prioritized since the time of exposure to enemy fire is minimized in such cases. Every unnecessary moment of exposure to enemy fire increases the risk of rescuers becoming victims themselves. If this happens, the number of potentially rescued casualties increases while the number of available tactical response forces decreases. This must be avoided at all costs, even if it means having to helplessly watch a person bleed out, who would have been easily saved under other circumstances. In light of this, a rescue attempt may need to be aborted during the approach to the wounded or even after reaching them due to sudden increased enemy pressure, leaving the patient to their fate because the risk to rescue teams becomes disproportionately high.
As mentioned earlier, emergency medical actions in the red zone/CUF are limited to applying tourniquets to stop life-threatening extremity bleeding. Depending on the algorithm used, only "M" (Massive Bleeding) or "C" (Critical Bleeding) is applied. The tourniquet should be applied as close to the body trunk as possible to cut off blood flow to the entire limb. This saves valuable time and ensures that any other severe bleeding injuries in the same limb not yet discovered also come under control and the limited medical resources available at the attack site are used as economically as possible. Due to the extreme hazard for both the wounded person and the rescuer, the alternative use of a pressure bandage is prohibited for tactical reasons. This measure would be considerably more time-consuming and would expose the wounded and rescuers to enemy fire for an unreasonably long time. Furthermore, there is a risk that a pressure bandage may loosen during further withdrawal and evacuation measures, leading to another significant blood loss event.
Although the use of a tourniquet by the first responder immediately at the unprotected attack site is generally prohibited, there are circumstances where this measure could be allowed. For example, if the wounded person is temporarily hidden from the attacker's view, for example, by a depression in the ground or behind a hedge. Moreover, in certain operational situations, there may be the possibility for security forces to momentarily shield the first responder from enemy fire using ballistic shields or protective blankets brought by security forces. This could provide them with the necessary time to stop extremity bleeding at the wounded person's location. The transfer of the injured person to a ballistic cover would immediately follow this initial medical action.
By now, the reader should realize the philosophy of tactical medicine can only be compared to traditional first aid or civil emergency medical response to a limited extent.
Yellow/Warm Zone - Tactical Field Care (TFC)
Treatment in the immediate vicinity of the attack site, without gunfire, in the (first) cover
Once the wounded person has been brought to the cover from the location and the first responders are no longer exposed to direct enemy fire, a more thorough examination of the wounded person can be carried out. Of course, sufficient ballistic cover is preferable to mere visual protection.
But what is considered sufficient ballistic cover? In layman's terms, it refers to a structural or natural protection that reliably stops projectiles used by the enemy, thus protecting us from direct gunfire. However, what reliably stops projectiles depends on several factors, such as:
- Type of weapons used by the enemy:
Short arms, long arms, machine guns, armor-piercing weapons, explosives
- Type of ammunition used by the enemy:
Caliber, charge, bullet shape, etc.
To stop gunfire from a small-caliber handgun, the driver's or passenger's door of an ambulance might be sufficient. After all, modern vehicle doors are equipped with various metal gadgets, such as electric window motors, side mirror adjustments, central locking systems, which can, in the best case, stop small projectiles of lighter calibers. However, a solid wall is usually not adequate protection against a grenade launched from a shoulder-fired rocket-propelled grenade launcher (RPG). And between a small-caliber pistol and a so-called rocket launcher (often used as a generic term for the entire category) lies a wide range of different weapon-ammunition combinations. Due to the proliferation and easy availability, it is expected that there will be an increased use of assault rifles based on the Soviet-Russian Kalashnikov platform by terrorist attackers in Germany. These weapons are reliable, inexpensive, and above all, widely available. Cautious estimates suggest there are 100 million copies of the numerous versions of the Automa...
Continue...
Red/Hot Zone - Care Under Fire (CUF)
Immediate measures at the scene of the attack under fire
From the armed opponent, there is an immediate danger to the life or limb of all those present on-site. This includes already wounded individuals, potential rescuers, as well as uninvolved individuals. In the red zone, unarmed emergency services personnel should not be present in principle. An exception would of course be accidental presence during an attack or a deliberate attack on emergency medical infrastructure, such as hospitals or ambulance teams.
The top priority for first responders in the red zone is the quickest possible avoidance of the present danger. This goal can be achieved by incapacitating the armed opponent. In other words, they are killed or seriously wounded so that they can no longer continue their actions. Another possibility would be for the offender to leave the scene due to the resistance. Depending on the scenario, it is also conceivable that the police forces may initially be unable to eliminate or displace the enemies. But they could support the evacuation of the wounded from the immediate danger area by providing covering fire. This is intended to keep the enemy down and allow evacuation teams to approach the wounded and transport them to suitable cover for further treatment.
This all requires coordinated action from the first responders. So they must return fire and communicate at the same time.
With the control center or similar:
Call for help. Where am I? How does the situation look like? Request reinforcements and rescue forces.
With your tactical unit:
A wounded colleague is at the front left at the corner of the house. Perpetrator with a long gun, entrenched behind a wall at 2 o'clock (in other words, from your location seen from the front right). Provide cover, I'll get the wounded.
With the wounded:
Crawl behind the corner of the house! How are you injured? Use your tourniquet! It's in your left leg pocket! We'll get you out as soon as we can!
In the red zone, the Care Under Fire phase, neutralizing the perpetrators is top priority as long as they can continue to hinder personnel at the attack site. As many personnel as possible must engage in the gunfight, with as few as necessary approaching the wounded. Medical measures are limited to the absolute essentials. Ideally, the wounded themselves seek cover and treat their injuries in the initial attack. Following the principle: If everyone helps themselves, everyone is helped. Stopping life-threatening, massive extremity bleeding by applying a tourniquet is, if anything, the only feasible emergency medical action in the red zone. And as noted above, ideally by the wounded themselves. If the victims of the attack are not trained gun carriers but unaware citizens, self-treatment is likely to be ruled out in most cases.
Essentially, it is crucial for the first responders to minimize the time spent at the immediate attack site. The top principle here is: "Do not burden your team by becoming a victim yourself!" This means that an approach to the wounded may need to be postponed if it poses a significant risk to the rescuer. Prioritization of casualties should be done before or during the approach, especially in scenarios with multiple casualties. Critically wounded individuals who are not in life-threatening conditions may need to be disregarded to treat those with a higher chance of survival, given the ongoing firefight. Triage is consciously avoided at this point since patient selection can only be very rough at this time and mainly occurs at a distance (remote assessment). It is conceivable that the nearest wounded individual to the rescuers is prioritized since the time of exposure to enemy fire is minimized in such cases. Every unnecessary moment of exposure to enemy fire increases the risk of rescuers becoming victims themselves. If this happens, the number of potentially rescued casualties increases while the number of available tactical response forces decreases. This must be avoided at all costs, even if it means having to helplessly watch a person bleed out, who would have been easily saved under other circumstances. In light of this, a rescue attempt may need to be aborted during the approach to the wounded or even after reaching them due to sudden increased enemy pressure, leaving the patient to their fate because the risk to rescue teams becomes disproportionately high.
As mentioned earlier, emergency medical actions in the red zone/CUF are limited to applying tourniquets to stop life-threatening extremity bleeding. Depending on the algorithm used, only "M" (Massive Bleeding) or "C" (Critical Bleeding) is applied. The tourniquet should be applied as close to the body trunk as possible to cut off blood flow to the entire limb. This saves valuable time and ensures that any other severe bleeding injuries in the same limb not yet discovered also come under control and the limited medical resources available at the attack site are used as economically as possible. Due to the extreme hazard for both the wounded person and the rescuer, the alternative use of a pressure bandage is prohibited for tactical reasons. This measure would be considerably more time-consuming and would expose the wounded and rescuers to enemy fire for an unreasonably long time. Furthermore, there is a risk that a pressure bandage may loosen during further withdrawal and evacuation measures, leading to another significant blood loss event.
Although the use of a tourniquet by the first responder immediately at the unprotected attack site is generally prohibited, there are circumstances where this measure could be allowed. For example, if the wounded person is temporarily hidden from the attacker's view, for example, by a depression in the ground or behind a hedge. Moreover, in certain operational situations, there may be the possibility for security forces to momentarily shield the first responder from enemy fire using ballistic shields or protective blankets brought by security forces. This could provide them with the necessary time to stop extremity bleeding at the wounded person's location. The transfer of the injured person to a ballistic cover would immediately follow this initial medical action.
By now, the reader should realize the philosophy of tactical medicine can only be compared to traditional first aid or civil emergency medical response to a limited extent.
Yellow/Warm Zone - Tactical Field Care (TFC)
Treatment in the immediate vicinity of the attack site, without gunfire, in the (first) cover
Once the wounded person has been brought to the cover from the location and the first responders are no longer exposed to direct enemy fire, a more thorough examination of the wounded person can be carried out. Of course, sufficient ballistic cover is preferable to mere visual protection.
But what is considered sufficient ballistic cover? In layman's terms, it refers to a structural or natural protection that reliably stops projectiles used by the enemy, thus protecting us from direct gunfire. However, what reliably stops projectiles depends on several factors, such as:
- Type of weapons used by the enemy:
Short arms, long arms, machine guns, armor-piercing weapons, explosives
- Type of ammunition used by the enemy:
Caliber, charge, bullet shape, etc.
To stop gunfire from a small-caliber handgun, the driver's or passenger's door of an ambulance might be sufficient. After all, modern vehicle doors are equipped with various metal gadgets, such as electric window motors, side mirror adjustments, central locking systems, which can, in the best case, stop small projectiles of lighter calibers. However, a solid wall is usually not adequate protection against a grenade launched from a shoulder-fired rocket-propelled grenade launcher (RPG). And between a small-caliber pistol and a so-called rocket launcher (often used as a generic term for the entire category) lies a wide range of different weapon-ammunition combinations. Due to the proliferation and easy availability, it is expected that there will be an increased use of assault rifles based on the Soviet-Russian Kalashnikov platform by terrorist attackers in Germany. These weapons are reliable, inexpensive, and above all, widely available. Cautious estimates suggest there are 100 million copies of the numerous versions of the Automa...
Continue...
SPARTANAT is the online magazine for Military News, Tactical Life, Gear & Reviews.
Send us your news: [email protected]
Ad
similar
Get the weekly SPARTANAT newsletter.
Your bonus: the free E-Book from SPARTANAT.